
Clinically trialled in over four thousand infants in over 36 clinical trials
Shown to increase Bifidobacteria levels in infant’s guts
Used in 120 neonatal intensive care units in affiliated hospitals across Japan, Australia, New Zealand and Singapore
Strain fact file
Microbiology profile:
Gram positive
Rod shape
Anaerobe
Non motile
Non spore former
GRAS certified in infants and food uses
Origin: Healthy human infant
Bifidobacterium breve M-16V® has been shown to:
Be safe in infants, including preterm babies
Increase levels of Bifidobacteria
Reduce the risk of necrotising enterocolitis (NEC) and infant mortality
Support the immune system
Reduce the risk of asthma or improve symptoms
Improve atopic dermatitis symptoms
May inhibit pathogens associated with colic
Key words: Probiotic, children, infants, newborn, immunity, gut health, bifidobacteria, colic
Introduction
The first three years of life are essential for microbiome and immune system development. These early years can shape our future health. Factors such as delivery mode (C-section or vaginal birth), gestational age, formula or breast feeding, and antibiotic use (Figure 1) can impact our microbiome which can increase the risk of present and future health issues.
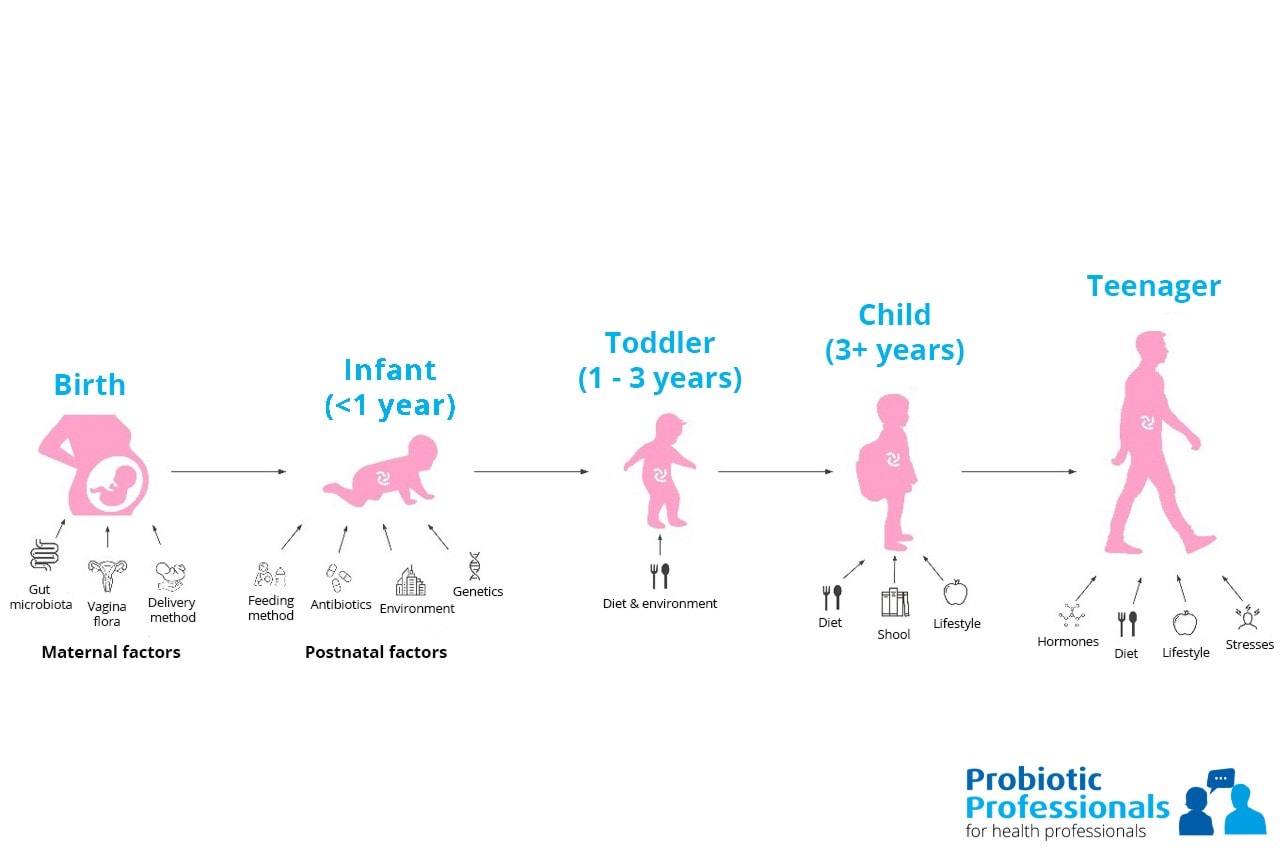
Figure 1. Factors affecting the infant microbiome (adapted from Tamburini S et al., 2016)
Bifidobacteria are a bacterial genus associated with immune regulation and digestive health. They are expected to dominate in a healthy infant’s gut. There are numerous studies highlighting their key role in infants for digestive support and immune modulation. Emerging research is additionally showing that the actual species of Bifidobacteria present is important. Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium bifidum and Bifidobacterium infantis should be present in high numbers (Wong B et al., 2019). Many strains belonging to these species can promote the barrier effect and competitively inhibit potential pathogens. These species also have the ability to break down human milk oligosaccharides (HMO’s), a highly selective prebiotic found in breast milk. During fermentation of HMO’s, they can produce short chain fatty acids which promote a healthy gut environment. In addition, these species may contain digestive enzymes such as ß galactosidases which help to break down lactose and other nutrients found in milk. (It should be noted that all of these abilities are strain specific). Good digestion and absorption of nutrients are essential in these early years due to infant growth and demanding energy requirements. This could explain the importance of Bifidobacteria and the microbiome in early years.
Bifidobacteria numbers are usually low in pre-term births, likely due to the many challenges these infants face from long stays in hospital, antibiotic use and possible enteral feeding. Typically, Bifidobacteria colonisation is delayed giving the opportunity for pathogenic bacteria to thrive with little competition in the gut. Enterobacteria and Streptococci are common colonisers in premature babies (Sakata H et al., 1985). This could explain why premature infants are at higher risks of infections, necrotising enterocolitis (NEC) or sepsis. Additionally, Bifidobacteria numbers may be lower in C-section babies which could explain why C-section babies are often at higher risk of asthma, allergies and metabolic diseases (Thavagnanam S et al., 2008).
It’s traditionally been thought that formula fed infants have lower numbers of Bifidobacteria, however recent research is showing that this may not be the case. Some studies have reported formula fed babies may have similar numbers of Bifidobacteria but it is not the dominant genus. There is proportionally less due to many other microbial genera being present, some potentially harmful (Lee SA et al., 2015). Additionally, the species of Bifidobacteria differ between breast fed and formula fed infants, with Bifidobacterium spp. in formula fed infants resembling species more commonly seen in adults (Turroni F et al., 2009). There is also some emerging research showing that Bifidobacteria species may also differ between C-section and vaginally born babies. It was found that Bifidobacteria colonisation occurred within three days of birth with B. bifidum and B. longum species dominating (Makino H., 2018) in vaginally born infants.
Colic commonly occurs in newborn’s. Colic has been associated with microbial imbalances, reduced diversity and inflammation. High levels of Escherichia spp. and Klebsiella spp. and low levels of Bifidobacteria have been associated with crying time in newborns (Dubois N et al., 2016) (De Weerth C et al., 2013). Therefore, rebalancing a baby’s microbiome by boosting levels of Bifidobacteria may reduce symptoms associated with colic.
This information provides researchers with a window of opportunity to intervene through the use of probiotics specifically formulated for an infant’s gut.
Survival & Safety
Bifidobacterium breve M-16V® has been demonstrated in clinical trials to be safe and can reach the gut alive. There have been numerous trials in preterm babies and those with necrotising enterocolitis (NEC) demonstrating the safety of the strain in vulnerable populations.
A gold standard trial in 2014, assessed B. breve M-16V® for its safety and ability to boost faecal B. breve counts in 159 preterm newborns (33 weeks or younger). They received either 3 billion colony forming units (CFU) of the probiotic or a placebo. They continued taking their respective supplement until 37 weeks old.
No adverse events were noted in the probiotic group during the trial period. B. breve counts significantly increased in stools of the probiotic group. This result gives strong evidence of the strain’s survival through the gastro-intestinal tract (Patole et al., 2014).
A meta-analysis conducted in 2017 analysed nine clinical trials (n=4840) regarding the use of B. breve M-16V® in preterm infants. The review found no adverse events through the use of the probiotic (Athalye-Jape G et al., 2017).
A randomised, controlled and double blinded study also assessed B. breve M-16V® for its tolerance and effect on growth in 211 infants. Full term infants who had not been breastfed for longer than one month were given either a control or synbiotic mix of 1.3 billion CFU B. breve M-16V®, galactooligosaccharides (GOS) and fructooligosaccharides (FOS). They took their respective supplement for 13 weeks. No adverse events were noted between the groups. Overall, the synbiotic combination supported adequate infant growth (Abrahamse-Berkeveld M et al., 2016).
One study assessed B. breve M-16V® counts in stool samples from 46 infants. B. breve M-16V® was taken daily (0.5 billion CFU) for six weeks. The study found B. breve M-16V® present in 85% of infants after six weeks (Ishizeki S et al., 2013).
Modulation of the infant microbiome
A baby biome should exhibit high levels of Bifidobacteria and lower numbers of Enterobacteria including Escherichia coli from birth. A delay in Bifidobacteria colonisation and dysbiosis may increase the risk of health conditions later in life.
A randomised controlled trial in 2004 found that B. breve M-16V® was able to significantly increase Bifidobacteria levels. The very low birth weight (VLBW) infants were split into three groups: 1) probiotic supplement approx 7.2 hours after birth, 2) probiotic supplementation approx. 36 hours after birth, and 3) the control group. The researchers found that group 1 had a Bifidobacterium dominant microbiome by week 2, compared with week 4 in group 2. No Bifidobacteria were found in the majority of group 3. Furthermore, in group 1, numbers of Enterobacteriaceae significantly decreased suggesting the strain was able to rebalance the microbiome of these infants (Li Y et al., 2004).
Another controlled study also found that 0.5 billion CFU of B. breve M-16V® increased Bifidobacteria levels in premature infants. Two weeks after birth, Bifidobacteria dominated the infant guts in the probiotic group. Whereas in the control group, higher levels of Bifidobacteria were not noted until week six (Akiyama K et al., 1994).
The randomised, controlled and blinded study by Patole et al., 2014 also showed increased Bifidobacteria, specifically B. breve species (Patole et al., 2014).
A synbiotic mixture of galactooligosaccharides (GOS) and fructooligosaccharides (FOS) alongside 18 million CFU of B. breve M-16V® was shown to significantly increase levels of Bifidobacteria in 129 children aged 1-3. The children received the synbiotic combination or a control for 12 weeks. Stool pH also decreased suggesting a more acidic environment had been created in which beneficial bacteria thrive. Stool consistency also improved in the synbiotic group (Kosuwon P et al., 2018).
Colic
High levels of Bifidobacteria may support overall health including digestion and immunity, but their numbers are also associated with happier temperaments (Aatsinki A et al., 2019). This may be part of the reason why a healthy microbiome may reduce the risk of colic.
A randomised, double blinded study found that B. breve M-16V® alongside prebiotics could increase levels of Bifidobacteria in C-section babies. A total of 153 infants born via C-section were randomised to receive either a synbiotic combination (B. breve M-16V® plus GOS/FOS), a prebiotic combination (GOS/FOS) or a control for 16 weeks. Infants born vaginally were used as a reference point. Infants were given their respective supplement from day 3-5 after birth. Bifidobacteria levels significantly increased in the synbiotic group from day five until week eight compared to the control, general increases were seen up to week 16 (Graph 1). Additionally, a significant reduction in Enterobacteria (including E. coli and Klebsiella spp.) was also noted (Graph 2). Additionally, the levels of Enterobacteria were higher in vaginally born infants than the synbiotic group by week 16.
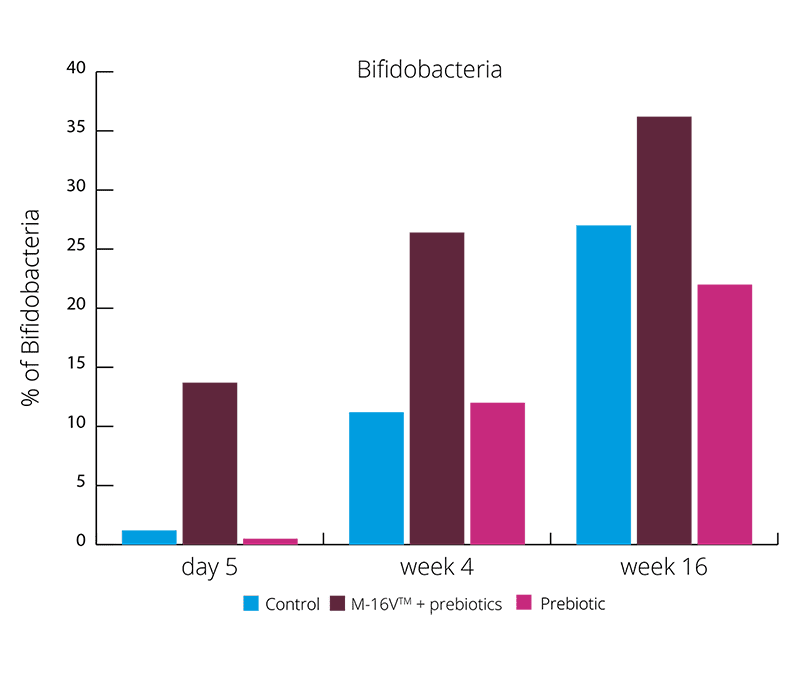
Graph 1 - shows the percentage of Bifidobacteria over a 16 week intervention period
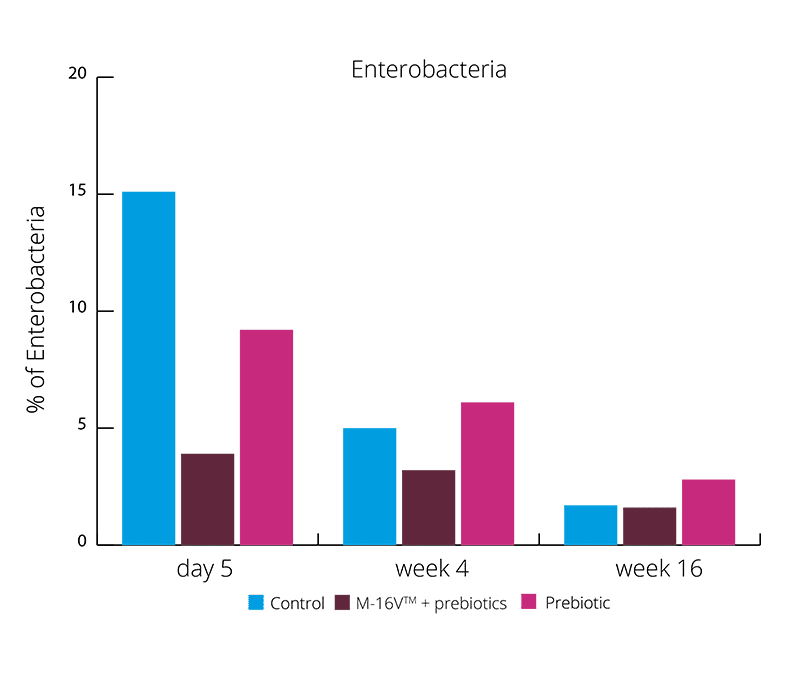
Graph 2 - shows the percentage of Enterobacteria over a 16 week intervention period
These results suggests the synbiotic group was able to create a more beneficial microbial balance. This is also supported by higher levels of acetate and lower faecal pH. (Chua MC et al., 2017). Increasing the levels of Bifidobacteria and reducing Enterobacteria may aid with colic symptoms. Vaginally born infants also suffer with colic, and these results showed the exhibited higher levels of Enterobacteria. B. breve M-16V® may be able to reduce the risk of colic in both vaginally and C section babies.
Premature infants and risk of NEC and infections
Use of probiotics in NICU’s is increasing. In some centres, probiotic use has seen NEC and infection rates drop significantly. Although premature birth complications are complex, it is postulated that many of these conditions are in some way related to the microbiome. As premature infants have immature guts with typically low levels of Bifidobacteria and high levels of inflammation this could be plausible.
A randomised controlled study found B. breve M-16V® was able to significantly reduce the risk of infection and sepsis in extremely and very low birth weight preterm infants. The study split 208 infants into a probiotic and placebo group. The probiotic group took 1 billion CFU of B. breve M-16V® from several hours after birth until discharge from the NICU. The authors concluded that B. breve M-16V® supplementation hours after birth may be an effective method to reduce the risk of infection and thus sepsis (Hikaru U et al., 2010).
A retrospective study analysed B. breve M-16V® for its ability to reduce NEC. The study included 564 infants who were split into probiotic and control groups. The probiotic group were given 1 billion CFU of B. breve M-16V® from birth to hospital discharge (37 weeks). In the probiotic group, no cases of NEC were recorded compared to six cases in the control group. Additionally, there was a significant reduction in infection and mortality from infection in the probiotic group compared to controls (Satoh Y et al., 2007).
A hospital in Australia conducted a retrospective cohort study analysing the effects of B. breve M-16V® in 1755 pre-term infants. The researchers analysed the incidence of NEC in pre-term infants for a period before probiotic intervention (2008-2010, n=835) and then after probiotic supplementation (2012-2014, n= 920). After B. breve M-16V® supplementation (three billion CFU) was given daily to preterm infants up until week 37. The researchers found when B. breve M-16V® was supplemented rates of NEC, NEC related mortality, late onset sepsis and age at full feeds significantly reduced in infants aged 28-34 weeks old. Reductions were also seen in infants aged 28 weeks or lower but these did not reach significance (Patole et al., 2016).
A potential theory to explain how B. breve M-16V® may decrease NEC incidence comes from the reduction of a short chain fatty acid (SCFA) know as butyrate. SCFA’s are produced by bacteria via the fermentation of undigested carbohydrates and proteins in the gut. They are generally associated with health and well-being but in preterm infants, overproduction may not be beneficial. Butyrate is produced from specific microbes in the gut such as Clostridia, Bacteroides and Escherichia spp. Butyrate may contribute to NEC in many different ways, from immune responses, inflammation and increased mucosal injury (Wang C et al., 2007).
A randomised controlled trial analysed the SCFA composition from stool samples of 66 preterm infants. They split the infants into groups depending on birth weight. Half of the infants in each group were given B. breve M-16V® whilst the others received no supplementation. After four weeks of probiotic supplementation, butyrate concentrations significantly decreased in the probiotic group (Wang C et al., 2007).
A randomised controlled trial assessed B. breve M-16V® effects on inflammation markers in pre-term infants. 2 billion CFU of B. breve M-16V® were given to preterm infant’s hours after birth. After four weeks, in the probiotic group, TGF-ß1 levels had significantly increased (Fujii T et al., 2006). TGF-ß1 is an important modulatory cytokine that has demonstrated anti-inflammatory effects and modulation of the cell cycle. The study didn’t analyse butyrate production, however high levels of inflammation are associated with NEC.
Additionally, by increasing levels of Bifidobacteria through B. breve M-16V® supplementation, this will help lower levels of butyrate via competition with butyrate producers alongside modulating inflammatory markers.
Immunity
During the early years, the microbiome helps to train the immune system, allowing it to develop and distinguish between friend and foe. Atopic dermatitis (AD) and asthma are heavily associated with one another and are often present in infancy. It’s been suggested that 40% of children with AD develop asthma in later childhood (Gustafsson D et al., 2000). Studies have shown that microbial imbalances in the gut may be associated with the onset of allergies and atopy. Low levels of Bifidobacteria and Lactobacilli and high levels of Escherichia coli and Clostridium difficile have both been associated with the development of eczema or atopy (Kalliomaki M et al., 2001) (Abrahamsson TR et al., 2012) (Melli L et al., 2016).
Atopic dermatitis (eczema)
Eczema rates in the UK are high. Majority of eczema cases are diagnosed by age 1 (Cork M J et al., 2019). Although the exact cause of eczema is unknown, there are likely to be many factors involved, including the microbiome. Increased gut permeability and imbalanced immune responses could contribute. The World Allergy Organisation (WAO) also took into consideration that probiotics for eczema may be beneficial (Fiocchi A et al., 2015).
A randomised controlled trial investigated B. breve M-16V® in 15 infants with eczema. They were split to receive either a probiotic or placebo and took their respective supplement for one month. In the probiotic group, researchers found significant improvements in the proportion of Bifidobacteria and allergic symptoms (cutaneous symptom score and total allergic score). The authors suggested B. breve M-16V® may improve eczema in infants (Hattori K et al., 2003).
Another randomised controlled trial was conducted assessing B. breve M-16V® in 17 infants with cow’s milk hypersensitivity and AD. After three months, the researchers found that B. breve M-16V® boosted Bifidobacteria and improved allergic symptoms from baseline results in the probiotic group. The researchers hypothesised that the strain may enhance regulation of the Th1/Th2 cell balance and improve cell integrity (tight junctions) that may have been compromised by milk allergies. The researchers also concluded that B. breve M-16V® is safe for infants with cow’s milk hypersensitivity (Taniuchi S et al., 2005). Another study also found that B. breve M-16V® could reduce the risk of occurrence of cow’s milk protein intolerances after small intestinal surgery (Ezaki et al., 2012).
A study in 2018 explored immune modulation in infants with moderate to severe AD. The study used samples from a previous randomised, blinded and controlled trial analysing a synbiotic mixture of B. breve M-16V® and GOS/FOS mix in 31 infants. AD has typically been associated with increases in Th2, Th22 and Th17 markers and high levels of CC chemokines. Results from this trial showed median SCORAD symptoms significantly decreased in both synbiotic and control groups, but more so in the synbiotic group. The researchers did note an increase in CXCL9 and reductions in Th1/Th2 ratios and stated that this data provides further understanding of B. breve M-16V® modes of action in AD (Hulshof L et al., 2018).
A study in 2014 looked at the effects of two probiotics, B. breve M-16V® and B. longum BB536 in 166 pregnant women and infants. The probiotic was given to the mothers one month before expected delivery and then given directly to the newborn for six months. Researchers found that in the probiotic group there was a significant reduction in the risk of eczema/AD development during the first 18 months of life (Enomoto T et al., 2014).
Asthma
Asthma is one of the most common health conditions, especially in children (Lin J et al., 2018). It is thought probiotics may support asthma due to immune regulation and modulation of inflammatory responses.
A double-blind, randomised placebo-controlled study trialled B. breve M-16V® in 75 infants (over 7 months old) with AD who were suffering with asthma like symptoms. The children were split into a synbiotic and placebo group. In the synbiotic group, infants received 1.3 billion CFU of B. breve M-16V® with a mixture of GOS/FOS. The infants received their respective supplement for 12 weeks, follow up analysis was conducted after one year. At follow up, the prevalence of ‘frequent wheezing’ was significantly lower in the synbiotic group than the control group (13.9% v 34.2% respectively) (Graph 3). Additionally, wheezing and/or noisy breathing apart from colds had significantly reduced in the synbiotic group compared with control (2.8% v 30.8% respectively) (Graph 3).
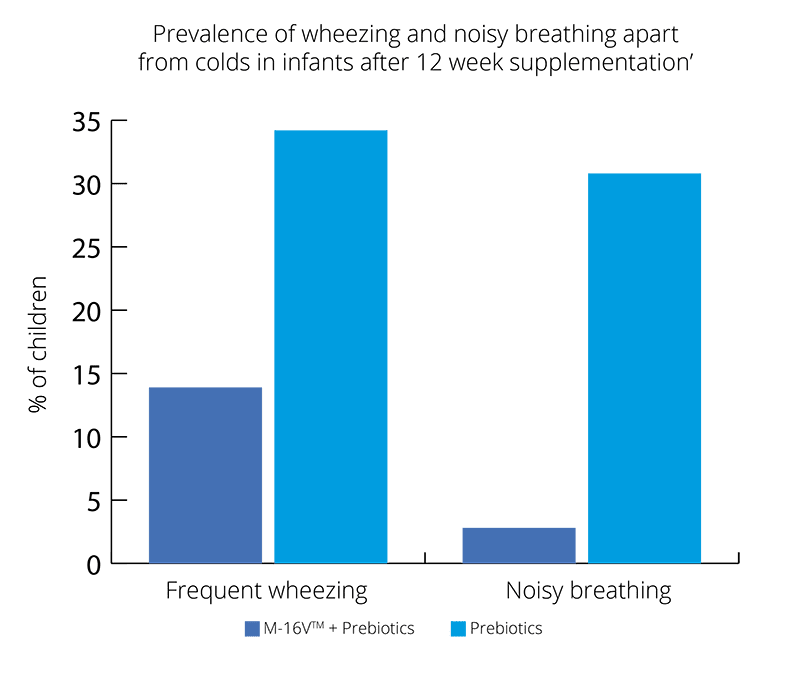
Graph 3 - supplementation with B. breve M-16V® significantly reduced both symptoms in infants with asthma like symptoms
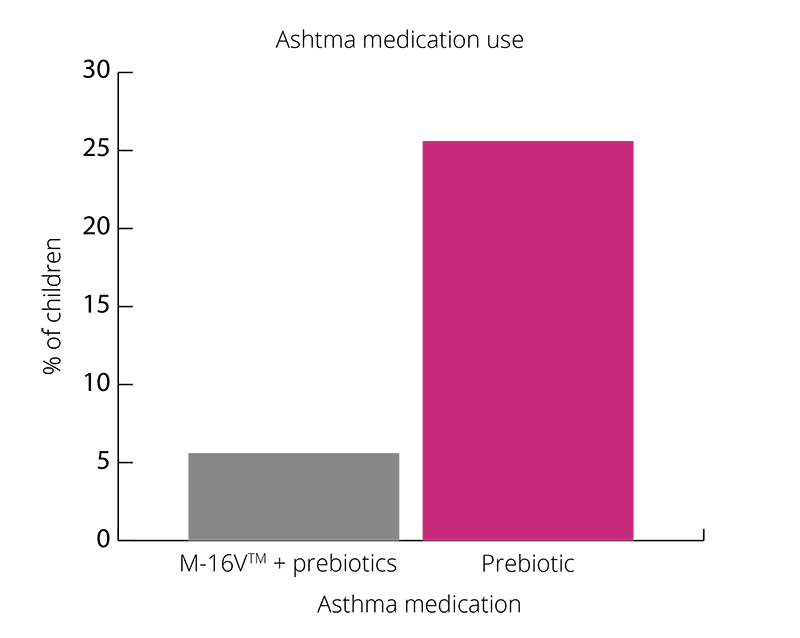
Graph 4 - shows a significant reduction in children starting asthma medication after baseline in the synbiotic group
Overall, results show promising results for B. breve M-16V® in children with asthma like symptoms (Van der Aa et al., 2011).
Another double-blind, randomised and placebo-controlled study investigated B. breve M-16V® in combination with two additional strains in 40 children with pollen induced, IgE mediated allergic rhinitis and intermittent asthma. Children in the probiotic group received 1 billion CFU of B. breve M-16V® alongside 3 billion B. longum BB536 and 1 billion B. infantis M-63. The children received their respective supplement daily for four weeks. Researchers found significant improvements in allergic symptoms and quality of life in the probiotic group (Del Guidice MM et al., 2017).
The exact mechanism for how B. breve M-16V® improves asthma and eczema symptoms is unclear. It is thought that it may be due to the ability of the strain to modulate the immune system and improve inflammatory responses and Th1/Th2 ratio.
General digestive issues
As well as promoting a healthy gut environment and microbiome. B. breve M-16V® may also support digestive symptoms.
A randomised, double blind and placebo-controlled study looked at a multi strain probiotic combination in 48 children (aged 11-16) with irritable bowel syndrome (IBS). The children were given either a control or a combination of B. infantis M-63, B. breve M-16V® and B. longum BB536. Children took their respective supplement for six weeks; they then had a two week wash out period and then swapped over to the other supplement. Abdominal pain significantly improved in children with IBS given the probiotic. Quality of life also significantly improved after probiotic consumption (48% in probiotic group compared with 17% in control) (Giannetti E et al., 2017).
Use in adults
B. breve M-16V® has been heavily researched for its probiotic benefits in infants. However, there are a few studies demonstrating its immune modulating effects in adults.
A double-blind controlled study analysed the effects of B. breve M-16V® in 24 adults with atopic dermatitis (AD). The participants were split into a probiotic (20 billion CFU) and placebo group, each group took their respective supplement daily for eight weeks. SCORAD symptoms and quality of life scores both significantly improved in the probiotic group. Bifidobacteria numbers also increased in the probiotic group. Although these results are promising, it must be that noted the symptom severity was less in the placebo group at the start. So further research is needed for B. breve M-16V® in adults with AD (Yoshida Y et al., 2010).
A randomised, blinded and controlled study also looked at the effects of B. breve M-16V® in 29 adults with asthma and house dust mite (HDM) allergy. The participants were split into two groups; probiotic and placebo. The probiotic group received 10 billion CFU of B. breve M-16V® alongside a galactooligosaccharide (GOS) and fructooligosaccharide (FOS) mix. After four weeks of supplementation, there were no significant differences in bronchial inflammation and asthmatic reactions between groups. However, there were significant reductions in Th2- cytokines and improved peak expiratory flow in the probiotic group (Van de Pol M et al., 2010).
Both these studies show promise for B. breve M-16V® use in adults with AD or asthma. However further research with higher numbers of participants is needed to fully understand the benefits.
Conclusion
B. breve M-16V® is a highly researched strain that has been trialled in thousands of infants. What makes this strain so unique is the extensive research in premature babies, highlighting its safety and efficacy. There is a clear interaction between B. breve M-16V® and the immune system, the strain has been shown to regulate inflammatory responses and help balance Th1/Th2 ratios, all helping to reduce atopy and allergies. The strongest clinical evidence lies in the strains ability to boost Bifidobacteria levels. It is probable that the strain is able to compete with pathogens residing in the gut and create an environment more favourable to indigenous beneficial bacterial strains. It would be of interest to conduct more randomised, controlled trials on the strain and to fully understand the mechanisms of action at play. All in all, the strain has demonstrated its ability to improve gut health, the microbiome and immune system in infants.
Authors: Information on this strain was gathered by Dr Kate Steed PhD Food and Microbial Sciences; Gut Microbiology (University of Reading), BSc Medical Microbiology; and Kerry Beeson, BSc (Nut.Med) Nutritional Therapist.
As some properties & benefits of probiotics may be strain-specific, this database provides even more detailed information at strain level. Read more about the strains that we have included from this genus below.
Bifidobacterium lactis strains: Bifidobacterium lactis Bi-07®, Bifidobacterium lactis BB-12®, Bifidobacterium lactis Bl-04®.
Bifidobacterium infantis strains: Bifidobacterium infantis 35624.
Bifidobacterium breve strains: Bifidobacterium breve M-16V®.