
Clinically trialled in pregnant and breastfeeding women
Research on postnatal depression and gestational diabetes
Often trialled alongside Bifidobacterium lactis HN019 and Lactobacillus acidophilus La-14®
A member of the Lactobacillus rhamnosus species
As of April 2020 L. rhamnosus has been officially reclassified to Lacticaseibacillus rhamnosus so the full strain name may also be referred to as Lacticaseibacillus rhamnosus HN001 (Zheng J et al., 2020).
Strain fact file
Microbiology profile:
Gram positive
Rod shape
Aerobic and anaerobic (facultative anaerobe)
Non spore former
GRAS & QPS safety status
Researched conditions:
Safety & survival
Post-natal depression & anxiety
Gestational diabetes
Immunity
Intimate health
Prenatal benefits to the baby
Researched in: pregnant women, newborns, infants, children, adults, elderly
Keywords: Probiotic, pregnant women, overall support
Introduction
Health during pregnancy is vital. Many pregnant women take supplements to support their babies’ health but may not realise that their own health can impact that of their baby’s both before and after birth. Research is highlighting the first thousand days of life to be essential in microbiome and immune system development. These first thousand days include the 270 days of pregnancy. Emerging research is showing probiotic supplementation from the first trimester onwards may have beneficial effects for both mother and baby.
The microbiome undergoes many changes throughout pregnancy. This is unsurprising due to the hormonal, immunological and metabolic changes that are happening. In the first trimester, both gut and vaginal microbiomes are relatively stable. From trimester 1 to trimester 3, more pronounced changes are seen.
There is a lot of research on the vaginal microbiome and pregnancy. Microbial imbalances in the vaginal tract have been associated with pre- term births and spontaneous abortions (Peelan MJ et al., 2019). Increased microbial diversity and vaginal infections, such as with Gardnerella spp or Candida albicans, have been associated with pregnancy complications (Selma- Royo M et al., 2019). It is thought they may lead to an increase in pro inflammatory cytokines and prostaglandins. This may stimulate uterine contractions and/or weaken foetal membranes. Fortunately studies have shown that the vaginal microbiome should become less diverse and lactobacilli dominant as the pregnancy progresses (Tamburini S et al., 2016) (Mesa M et al., 2020). This could be due to the rise in oestrogen. High oestrogen levels are associated with higher levels of glycogen in the vaginal tract, a major food source for lactobacilli. Lactobacilli can offer many protective effects against infections including the production of lactic acid, antimicrobials, and bio surfactants. These will all help to create an environment that is less favourable to pathogenic microbes thus inhibiting their growth. One study found that pregnant women in the last trimester had significantly different vaginal microbiomes to non pregnant women. Pregnant woman had higher levels of lactobacilli including Lactobacillus vaginalis, Lactobacillus crispatus and Lactobacillus jensenii. Whilst non pregnant woman exhibited a more diverse microbiome (Romero R et al., 2014).
There is little research on the gut microbiome changes throughout pregnancy, most studies focus on the vaginal, placental, and oral microbiomes. However, a study in 2012 found that pregnant women in trimester three exhibit gut microbiomes similar to that of individuals with diabetes or metabolic syndrome (Koren O et al., 2012). In the study, the scientists transferred stool samples from women in their first and third trimester into germ free mice. Stool from the first trimester resulted in little changes to the mouse. However, stools from the third trimester saw the mice gain weight, have insulin desensitisation and a different microbiome to that from trimester one. Further microbiome analysis of trimester one and three, showed as pregnancy progressed the microbiome reduced in diversity. The microbiome from trimester one resembled that of a healthy non pregnant woman. By trimester three, there were increases in inflammatory bacteria such as Proteobacteria, decreases in butyrate producers and increases in bacteria that give higher energy yields. Since this study, few studies have been conducted to confirm these results. If we do see these changes, we can conclude that this forms part of a normal pregnancy. The problems can arise if a woman is already predisposed to diabetes, in which case her risk of gestational diabetes is higher.
Microbiomes from the gut and vaginal microbiome likely transfer to the baby during labour. This explains why infants born from C sections and vaginal routes exhibit different microbiomes (Sheo Y et al., 2019). It is therefore important for expectant mothers to take care of the microbiomes during pregnancy. Diet, lifestyle, antibiotics, stress levels can all impact the microbiome which can result in dysbiosis and reduced passage of beneficial bacteria to the newborn.
Post labour, it’s been shown that vaginal and gut microbiomes may take time to return to ‘normal’ after birth. For the gut microbiome, it’s been estimated to take one month (Koren O et al., 2012). However, a study in the vaginal microbiome showed differences up to a year post birth (DiGiulio D et al., 2015) . However, instead of lactobacilli dominating, vaginal samples were abundant in many gut microbes suggesting migration during labour. This may increase the risk of intimate infections post pregnancy. There is also some evidence to suggest that post-natal depression may affect the quality of microbes present in breast milk which are passed to the new born (Browne P et al., 2019).
Therefore, health and well-being during pregnancy and postnatally is vital for women.
Safety and survival
Human clinical trials on L. rhamnosus HN001 conducted in expectant mothers and during breastfeeding have shown no adverse effects on birth outcome; and no other adverse effects have been reported. This is highlighted throughout the assessment of trials in this review.
A study in 2009, assessed L. rhamnosus HN001 purely for its safety profile in newborns and pregnant women. The gold standard study included 500 pregnant women. They received L. rhamnosus HN001 or placebo from 35 weeks of gestation and continued taking up to six months post birth. New-borns also took the strain directly from birth up to two years. The researchers found the strain was well tolerated with no significant differences between the probiotic and control groups (Dekker J et al., 2009).
A gold standard study found increased levels of L. rhamnosus in stools during supplementation for two years. Infants were split to receive either L. rhamnosus HN001, B. lactis HN019 or placebo daily for two years from birth. Mothers also received a respective supplement from 35 weeks gestation until six months post birth if breastfeeding. L. rhamnosus levels in stools were boosted throughout L. rhamnosus HN001 supplementation from three months to two years. This was significantly more than L. rhamnosus levels in the B. lactis HN019 and placebo groups (Wickens K et al., 2008).
Postnatal depression and anxiety (PND)
The gut-brain axis is an exploding research area connecting our mental health, well being and behaviour to our microbial profile. Our microbiome may be able to interfere with neural pathways, neurotransmitter production and metabolism and central nervous systems. Postnatal depression is thought to affect approximately 10-15% of women (NHS, 2011). This number is predicted to be even higher as many woman often don’t realise they have it or do not report it. L. rhamnosus HN001 has been shown to reduce PND in mothers.
A gold standard study showed L. rhamnosus HN001 was able to significantly reduce postnatal depression and anxiety. The study included 380 women at 14-16 weeks gestation. They were randomised to receive either a daily dose of 6 billion CFU’s of L. rhamnosus HN001 or a placebo for the remaining duration of pregnancy and for six months post birth whilst breastfeeding. Mothers in the probiotic group reported significantly lower depression (Graph 1) and anxiety scores. Interestingly, infant colic was associated with higher depression scores (no significant differences between probiotic or control group). (Slykerman et al, 2017).
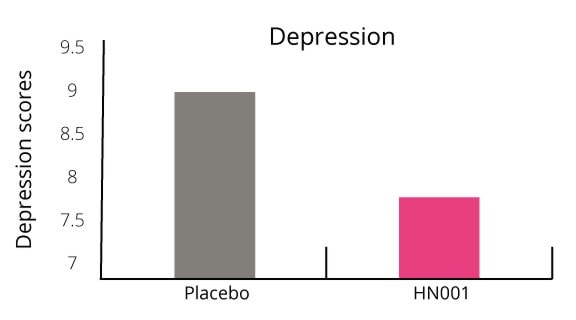
Graph 1 - L. rhamnosus HN001 was able to significantly reduce depression scores in women post-birth
Additionally, the number of women who scored above the cut off point for clinical anxiety was 50% lower in the probiotic group (Graph 2). Only 15.6% of women suffered with clinical anxiety in the probiotic group compared with 29.4% in the placebo group.
This is one of the first studies to show an association between probiotic use and postnatal depression.
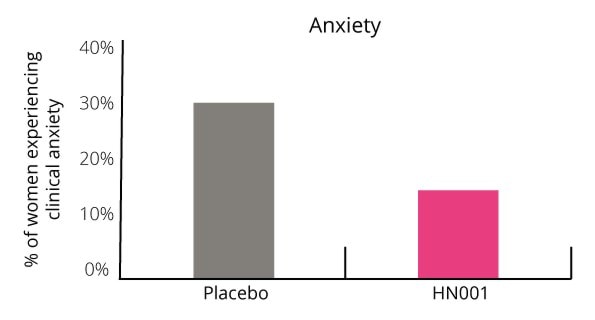
Graph 2 - shows L. rhamnosus HN001 halved the number of women suffering from clinical anxiety
Gestational diabetes (GDM)
It is estimated that 8-24% of pregnant women may develop GDM (Farrar D et al., 2016). This risk can vary depending upon family history, previous GDM diagnosis, age, weight preconception and ethnicity. The microbiome may contribute to GDM due to the microbial changes outlined in the study by Koren et al., (Koren O et al., 2012). L. rhamnosus HN001 has been shown to reduce the risk of GDM, especially in pregnant women more at risk.
An additional paper was published using the original 380 women and study design from the postnatal depression study. The only difference was this research looked at GDM rates. As before, the gold standard study included 380 women who were split to receive either L. rhamnosus HN001 or placebo from 14-16 weeks gestation to six months post birth. GDM was assessed at 24-30 weeks. There was a general trend in the reduction of GDM in the probiotic group (Graph 3). However, L. rhamnosus HN001 significantly reduced GDM rates in women over the age of 35 and in women with a history of GDM (Graph 4).
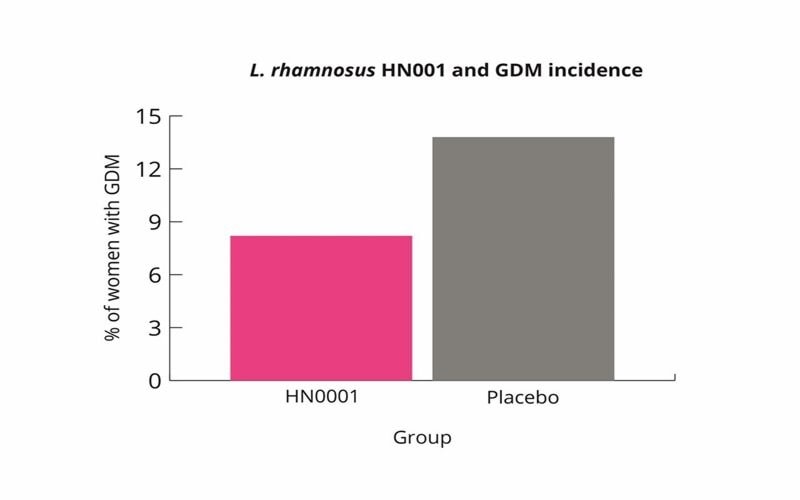
Graph 3 - shows reduction in GDM rates after receiving L. rhamnosus HN001 supplementation
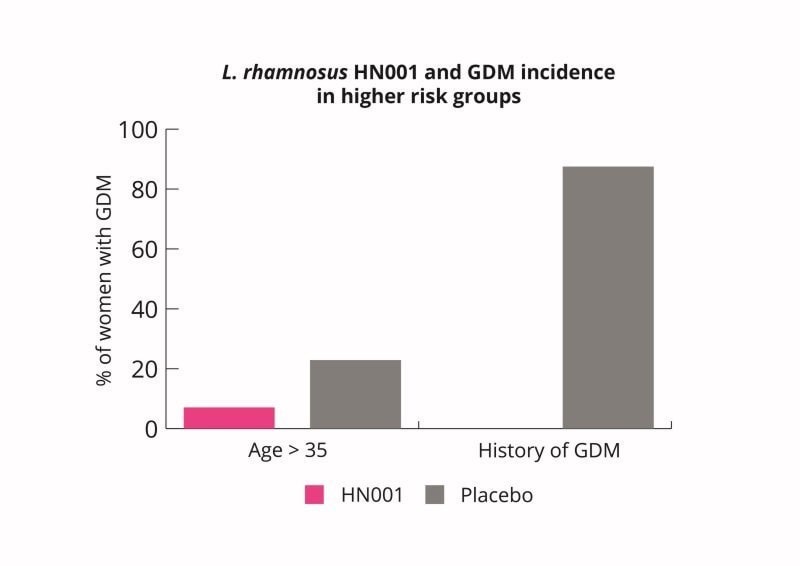
Graph 4 - shows significant reductions in GDM rates in women at higher risk after L. rhamnosus HN001 supplementation
L. rhamnosus HN001 supplementation may therefore be a useful intervention for pregnant women to lower their risk of GDM. L. rhamnosus HN001 supplementation may be especially useful for woman at higher risk (Wickens K et al., 2017).
Immunity
L. rhamnosus HN001 may enhance pregnant women’s immunity but it may also have some indirect benefits to foetal and/or newborn immune development.
A study in 2001 demonstrated L. rhamnosus HN001 was able to enhance phagocytic activity and NK cell activity in 52 healthy participants (Sheih Y et al., 2001). This immune enhancing ability of L. rhamnosus HN001 has also been demonstrated in murine studies (Gill et al., 2001) (Gill et al., 2000).
A randomised controlled trial was conducted on pregnant women in their last trimester. Women were split into three groups to receive either 6 billion CFU of L. rhamnosus HN001, 9 billion CFU of B. lactis HN019 or a placebo. They took their respective supplement from 2- 5 weeks before delivery and continued for 6 months post birth. In both probiotic groups, cytokine IFNy was significantly higher in the cord blood compared with the placebo group. However, in the L. rhamnosus HN001 group, IFNy was significantly higher than in the B. lactis HN019 group. TGF- beta levels in the breast milk were significantly higher in both probiotic groups compared to placebo. IgA in the breast milk was also significantly higher after probiotic supplementation. This study demonstrates that maternal supplementation of L. rhamnosus HN001 may have protective immune effects (Prescott SL et al., 2008). Higher levels of IFNy in cord blood have been associated with protective effects in allergic diseases such as asthma, wheezing and sensitisation (Macaubas C et al., 2003).
Intimate health
Promoting good vaginal microbial health during pregnancy is important. Imbalances in the vaginal microbiome can lead to serious outcomes. Many pregnant women often suffer with intimate issues including bacterial vaginosis. This often requires a course of antibiotics which could impact the baby’s health. Antibiotic use in pregnancy has been shown to increase the risk of asthma, allergies and eczema in children (Risnes KR et al., 2011) (Hoskin-Parr L et al., 2013).
A gold standard study analysed whether L. rhamnosus HN001 was able to support vaginal health in 40 women. Participants received either a combination of L. rhamnosus HN001, Lactobacillus acidophilus La-14® (10 billion CFU/day) and lactoferrin or a placebo for 14 days. They took their respective supplement orally, twice daily. Vaginal swabs showed an increase in L. rhamnosus and L. acidophilus levels on day 14 and 21. No adverse events were noted from probiotic supplementation. The study strongly suggests that both strains are safe and able to colonise in the vaginal tract when taken orally (DeAlberti D et al., 2015).
Another gold standard study analysed the effects of L. rhamnosus HN001 in 40 women with intermediate bacterial vaginosis. Women received either a combination of L. rhamnosus HN001, Lactobacillus acidophilus La-14® (5 billion CFU/day) and lactoferrin or placebo for 15 days. Vaginal swabs were collected at baseline and day 15. Increases in L. rhamnosus and L. acidophilus levels were detected by day 15 in the probiotic group. Baseline Nugent scores were 5.09 and 5.10 in the probiotic and placebo group respectively. After the intervention period, in the probiotic group, the Nugent score had significantly reduced to 2.9, which is considered to be a non BV score (Graph 5). This compared with a Nugent score of 5.14 in the placebo group, indicating no placebo effect. The probiotic group also exhibited significant improvements in itching and discharge (Graph 6).
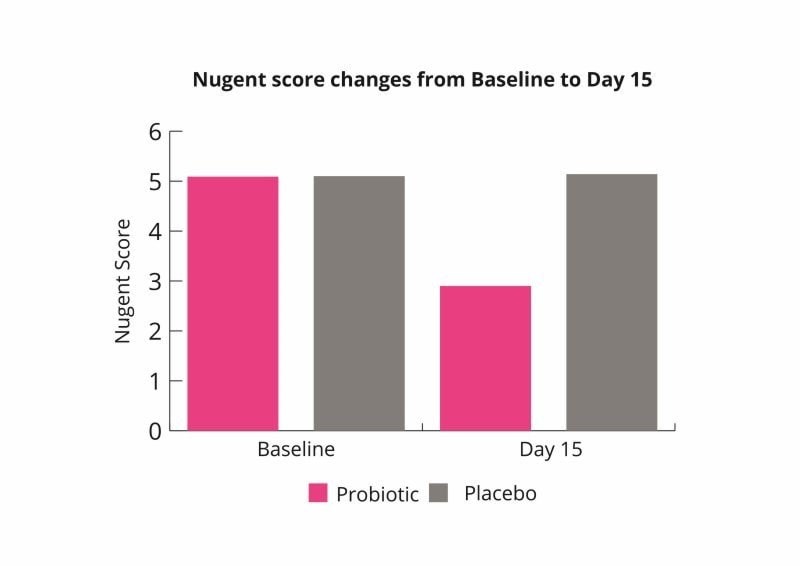
Graph 5 - shows L. rhamnosus HN001 administration led to significant improvements in Nugent scores from baseline
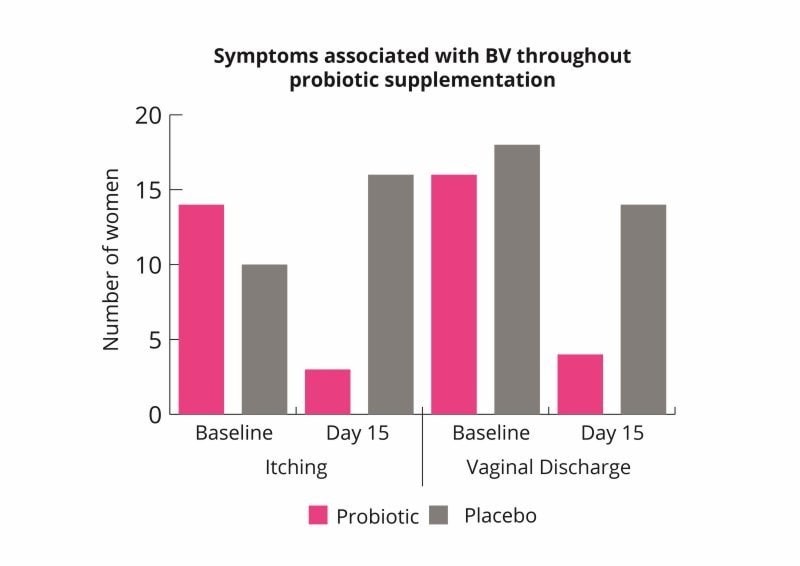
Graph 6 - shows fewer women exhibited symptoms in the L. rhamnosus HN001 group compared with placebo
These results indicate that the probiotic combination may help to rebalance the vaginal microbiome and improve symptoms of bacterial vaginosis (Russo et al., 2019).
A randomised clinical trial analysed the effects of L. rhamnosus HN001 in 48 women with thrush. All women tested positive for Candida albicans and exhibited thrush symptoms. Women were randomised to receive a combination of L. rhamnosus HN001, Lactobacillus acidophilus La-14® and lactoferrin or placebo. They took two capsules (10 billion CFU) daily for 5 days followed by one capsule (5 billion CFU) daily for 10 days per month, for six months. They started the two capsules on the first day of their menstrual cycle. Before probiotic or placebo supplementation started, during the induction phase, all women were treated with clot****zole for a week. By 3 months, only 8.3% of women in the probiotic group had itching compared to 70% in the placebo group. By month 6, no women had itching in the probiotic group compared with 83.3% in the placebo group. The study also found significantly improved vaginal discharge, cure and recurrence rates in the probiotic group. Only 28.2% of women had recurrences at six months, compared with 100% in the placebo group. The study demonstrated the effects of the probiotics to inhibit C. albicans growth thus reducing symptoms and recurrence rates (Russo et al., 2019).
Another gold standard study similar to the design in the trial above (Russo et al., 2019) looked at the effects of L. rhamnosus HN001, Lactobacillus acidophilus La-14® and lactoferrin on bacterial vaginosis over the course of the menstrual cycle, with an initial dose of metr*****zole. The six month study in 48 women (split into a placebo and probiotic group) found significant improvements in vaginal discharge, itching and cure rates in the probiotic group (Graph 7).
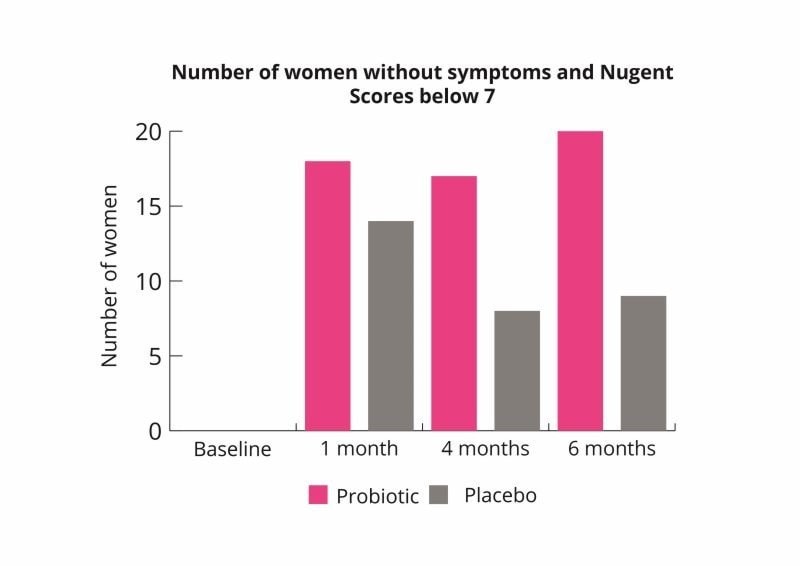
Graph 7 - highlights the ability of L. rhamnosus HN001 to improve the vaginal microbiome
Eczema
Eczema is very common in infants and has been associated with microbial imbalances in the gut and inflammation. Some studies have shown that probiotic supplementation to the mother followed by giving directly to the newborn may reduce the risk of eczema. Three studies followed up on one another (forming a six year study) found L. rhamnosus HN001 had significant benefits on the reduction of eczema.
The first study was conducted in 2008. This gold standard study looked at the effect of two probiotic strains and their ability to prevent eczema. The study included 474 pregnant women who were randomised to receive either; 9 billion CFU of B. lactis HN019, 6 billion CFU of L. rhamnosus HN001 or a placebo daily from 35 weeks gestation. They continued taking their respective supplement until 6 months post birth if breast feeding. Newborns were given the same supplement as their mother from birth to two years of age. During the two years, prevalence of eczema and common allergens were monitored. Little effects were seen in the B. lactis HN019 group. However, L. rhamnosus HN001 group was able to halve the number of infants who developed eczema (14% v 27% in placebo). Both IgE- associated and non IgE associated eczema reduced, however the effect was only significant for IgE- associated eczema. L. rhamnosus HN001 also showed a protective effect against the severity of eczema, with significantly fewer SCORAD scores over 10. The results highlight that pre natal supplementation could play an important role in infant eczema development. The results also highlight strain specificity, although B. lactis HN019 has excellent results for indications, there was little benefit in its consumption for eczema (Wickens K et al., 2008).
Due to the promising results seen and protective effects of L. rhamnosus HN001, follow up studies were conducted.
This first follow up was after two years, in which 425 of the initial 474 children participated (90%). The presence and severity of eczema were assessed, as well as symptoms of asthma (parent reported). Children from the L. rhamnosus HN001 group were still significantly less likely to have developed eczema by age four. There was a general protection against developing higher SCORAD scores, but this was not significant (P=0.09). Atopic sensitisation was also lower in the L. rhamnosus HN001 group, but also did not reach significance (P= 0.09). The risk of rhinoconjuctivitis was also significantly lower in the L. rhamnosus HN001 group. No protective effects were seen in the B. lactis HN019 or placebo groups (Wickens K et al., 2013).
The second follow up was conducted four years after the original study in 2008 (four years post supplementation). Nearly all children participated in this follow up (n=422, over 85% per group). Prevalence and severity of eczema were assessed alongside atopic sensitisation and questionnaires for asthma, wheeze and rhinoconjuctivitis. Children in the L. rhamnosus HN001 group, once again saw a significant protective effect against eczema development. Interestingly in the L. rhamnosus HN001 group, SCORAD symptoms over 10 had significantly reduced, as well as skin prick sensitisations. The protective effect against rhinoconjuctivitis were not maintained in this follow up. Overall the analysis show L. rhamnosus HN001 was able to reduce the cumulative prevalence of eczema by 40% and SCORAD values above 10 by 30%. As well, as L. rhamnosus HN001 reduced the risk of developing SPT sensitisation. It was proposed that L. rhamnosus HN001 was able to exert its protective effects by enhancing cell integrity and gut barrier function and providing a more balance Th1/Th2 ratio (Wickens K et al., 2013)
Overall L. rhamnosus HN001 supplementation in the later part of pregnancy and direct supplementation to the infant from birth for two years was able to reduce the risk of eczema up to the age of six. This highlights the importance of the first few years of life. It provides a window of opportunity to intervene with probiotics to potentially reduce health conditions such as eczema and allergies.
Conclusion
Probiotic supplementation in pregnancy is an emerging area of research due to the importance of maternal health during gestation. Overall L. rhamnosus HN001 has been demonstrated to support many aspects of a woman’s health and wellbeing. It has been trialled extensively in pregnant women showing safety and efficacy. L. rhamnosus HN001 is one of the few strains to demonstrate abilities supporting mental well-being, vaginal health and immunity.
Authors: Information on this strain was gathered by Dr Kate Steed PhD Food and Microbial Sciences; Gut Microbiology (University of Reading), BSc Medical Microbiology; and Kerry Beeson, BSc (Nut.Med) Nutritional Therapist.
As some properties & benefits of probiotics may be strain-specific, this database provides even more detailed information at strain level. Read more about the strains that we have included from this genus below.
Lactobacillus acidophilus strains: Lactobacillus acidophilus LA-05, Lactobacillus acidophilus NCFM®, Lactobacillus acidophilus Rosell-52.
Lactobacillus casei strains: Lactobacillus casei Shirota, Lactobacillus casei DN-114001.
Lactobacillus plantarum strains: Lactobacillus plantarum LP299v.
Lactobacillus reuteri strains: Lactobacillus reuteri Protectis and Lactobacillus reuteri RC-14®.
Lactobacillus rhamnosus strains: Lactobacillus rhamnosus LGG®, Lactobacillus rhamnosus HN001, Lactobacillus rhamnosus GR-1® and Lactobacillus rhamnosus Rosell-11.
Lactobacillus paracasei strains: Lactobacillus paracasei CASEI 431®.